CLINICAL CASE
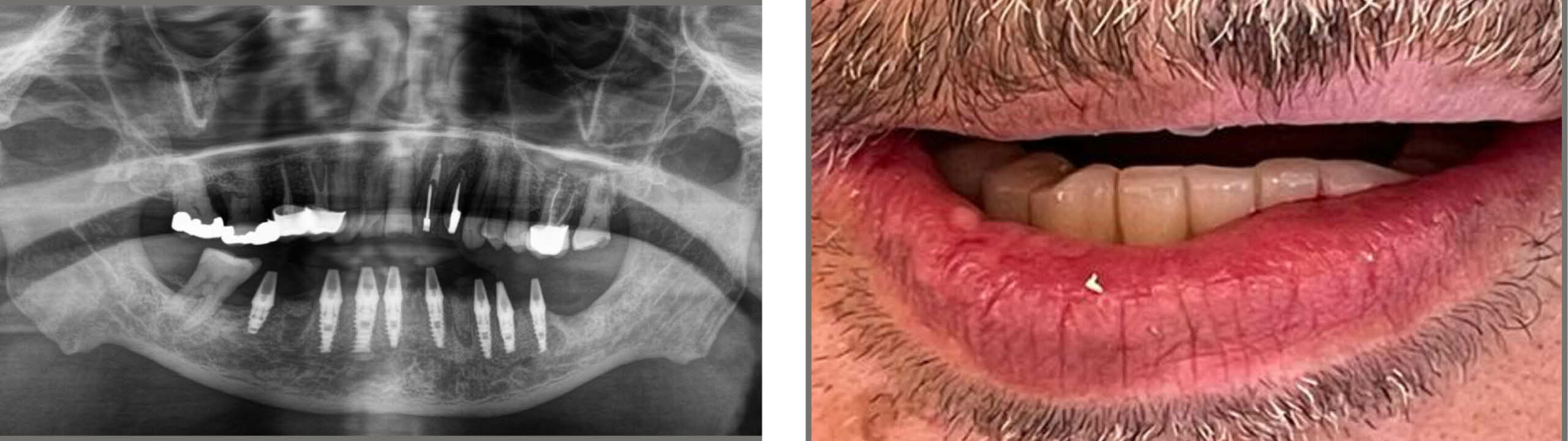
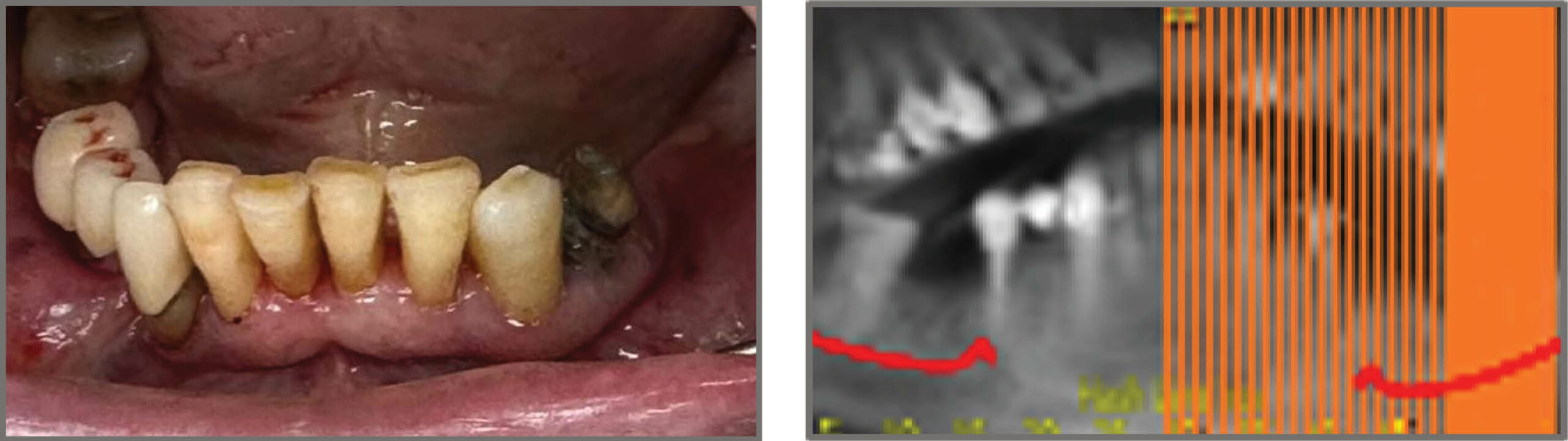
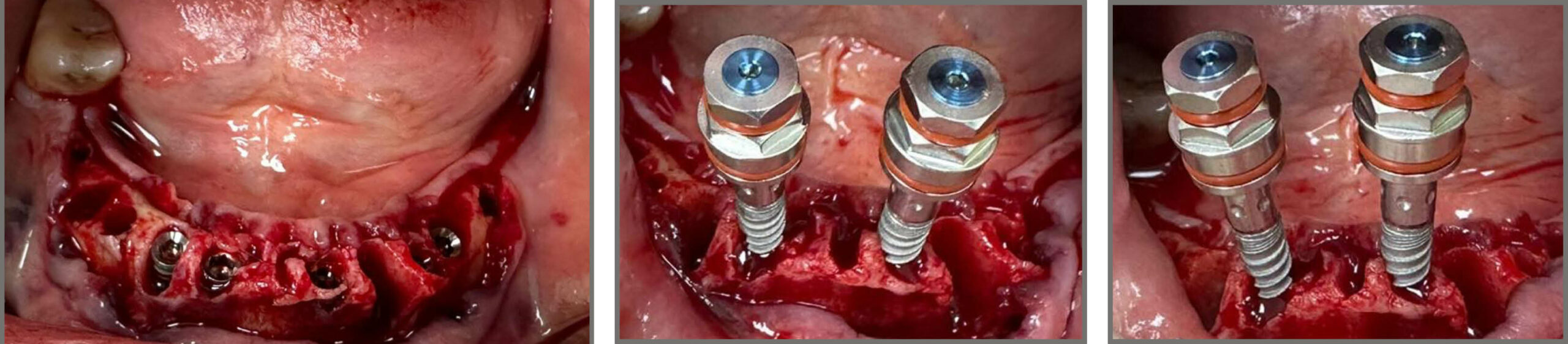
A 52-year-old man comes to our clinic with generalized severe chronic periodontitis, hopeless 45-33 teeth. He underwent a clinical examination, photographs, a complete RX series, and a CT scan. We planned to do periodontal treatment that includes initial preparation, root planning, and re-evaluation after 1 month., later extraction of teeth 45-33 and immediate placement of TUFF classic implants in area 46-36. Given the demands of the patient to have teeth immediately and not to wait too long to finish the whole treatment, leads us to choose immediate implantation and loading combined with bone augmentation. Because of narrow bone and large bone defects, we decided to operate with an open flap and not flaless procedure. After the initial preparation, we proceeded to extractions and the 8TUFF implant placement surgery that we had planned. All of them are placed with a minimum torque of 40Ncm so we can use the lower implants to support the cemented-retained provisional immediate prosthesis that the patient will wear. The patient’s mouth is scanned with a Sirona scanner and sent to the laboratory where a PMMA prosthesis is manufactured and placed in the patient after the implantations.

TREATMENT PLAN
- Periodontal treatment and re-evaluation
- Extraction 45-33
- Immediate implantation of 8 TUFF implants
46-44-43-42-32-34-35-36

- Bone augmentation – in the sockets between the implants and the buccal plates and buccal to all the ridges using bovine bone and CA-SULPHATE (Bond appetite)
- Immediate loading with PMMA bridge 46-36
- Final rehabilitation – 46-36 screw-retained zirconia bridge
Surgical procedure
- Extractions 45-33
- Drill 2 mm – guiding pins and parallel examination
- Palatal position and inclination
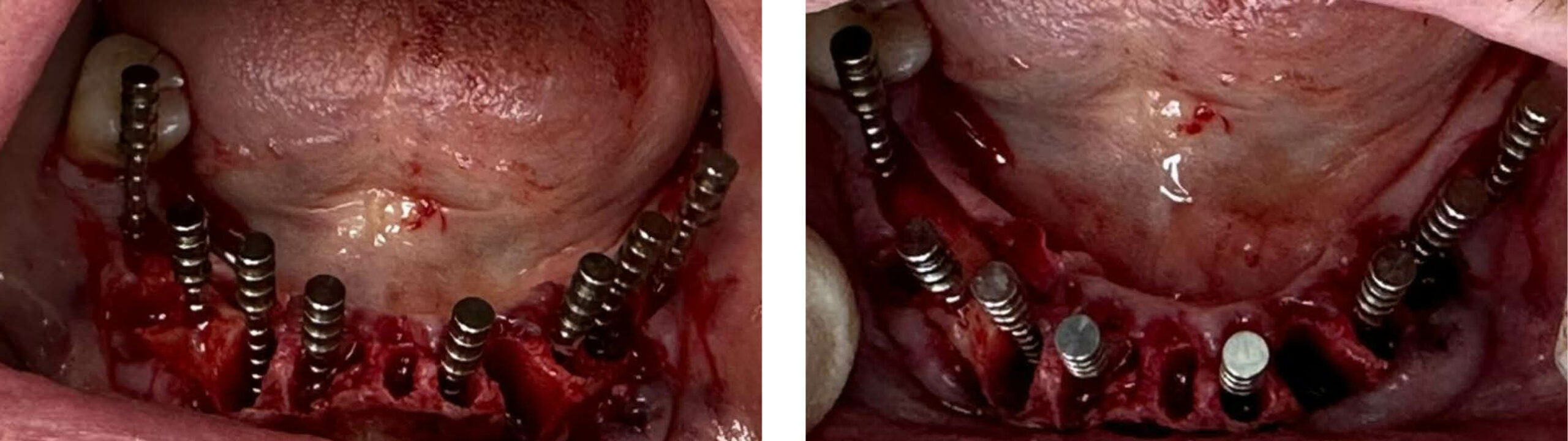
- Placing 8 Tuff implants – 5 X 3.75/11.5 (42 42 44 32 34) , 2X 3.75/10 (35 36) , 1 X4.2/6 (46)
- Drill 2.8 mm – 3.2 mm only expanding the coronal part of the osteotomy
- Palatal position and inclination
- Buccal bone defect 43, 33
treated by Placing bovine
bone all over the buccal
ridge and then cover the
bone with ca-sulphate.
- Insertion tourqe > 40 Ncm

DISCUSSION
The success of the procedure depends on the skill of the clinician since it is not an easily used technique and not all surgeons know how to perform it. On the other hand, late implants are much easier to place, since their use has become very widespread in recent years, and they have become a conventional treatment.
Even so, for the teeth in a-day cases, the clinician must also have certain skills, since we are talking about cases of large bone atrophies where the placement of conventional implants is done with regenerative techniques of certain complications, such as vertical and horizontal bone augmentations, soft tissues repairs and flapless surgeries.
Therefore, the level of skill may be an important point in determining between one technique and another, but it is by no means a determining factor.
On the other hand, we believe that time can be a more determining factor since nowadays, the demands of our patients are increasingly greater. If we place immediate implants, we could have the complete rehabilitation finished, with a definitive prosthesis, in 4/5 months, while late implants with bone grafts would take longer than that time.
In addition, the indisputable advantage of being able to wear a fixed temporary prosthesis from the first moment, while, if we perform late implants, the only prosthesis we could use would be a removable one, and not in all cases.

Summary and conclusions
- Immediate implantation and loading is the treatment of choice if it is possible according to the diagnosis
- The surgery for narrow ridges and large bone defects has to be done with an open flap. The procedure is very technique-sensitive and hence high surgical skills are needed
- The position of the implants is the key factor for the best clinical and aesthetic results
- Immediate implantation and loading procedures `have very high success rates the same as conventional implantation and even higher as mentioned in most implant journals